
Constipation is one of the most common bowel symptoms and can be divided by the cause of the symptoms into primary and secondary constipation.
Primary constipation can be functional or idiopathic constipation, slow transit constipation (STC).
Secondary constipation can be caused by a number of factors. It may be due to pharmacological reasons, a medical condition (for example Hirschsprung, MS, Parkinson), and/or mechanical obstruction such as rectal stricture, rectocele, or a bowel obstruction.
Primary or Functional constipation is common, and prevalence is estimated between 2-28% of the population. The elderly and those of lower socioeconomic status are particularly affected. Constipation is 10 times more frequently reported in women than in men.
Functional constipation is generally considered to be harmless in the medical sense, i.e. it does not cause any organic damage nor shorten life expectancy. However, it is common that quality of life is reduced due to the burden of the symptoms.
Refractory constipation is described when symptom relief is not achieved after a given time period of treatment.
Slow transit constipation (STC) or colonic inertia is defined as severe functional constipation without any pelvic floor dysfunction. STC is diagnosed together with radiographic evidence of delayed transit with physiologic absence of colonic motor activity and no response to pharmacological stimulation during colonic motility recording. About 15 to 30% of constipated patients have slow transit constipation. Essentially it occurs because peristalsis within the colon is greatly reduced and the ability for stools to move along the bowels becomes very slow. The reason for this reduced movement is poorly understood. Some theories suggest a lack of fiber in the diet, autonomic neuropathy, and disorders of both the enteric nervous system and the endocrine system.
Assessment, diagnosis and treatment of constipation needs to be tailored for each individual person.
Treating constipation
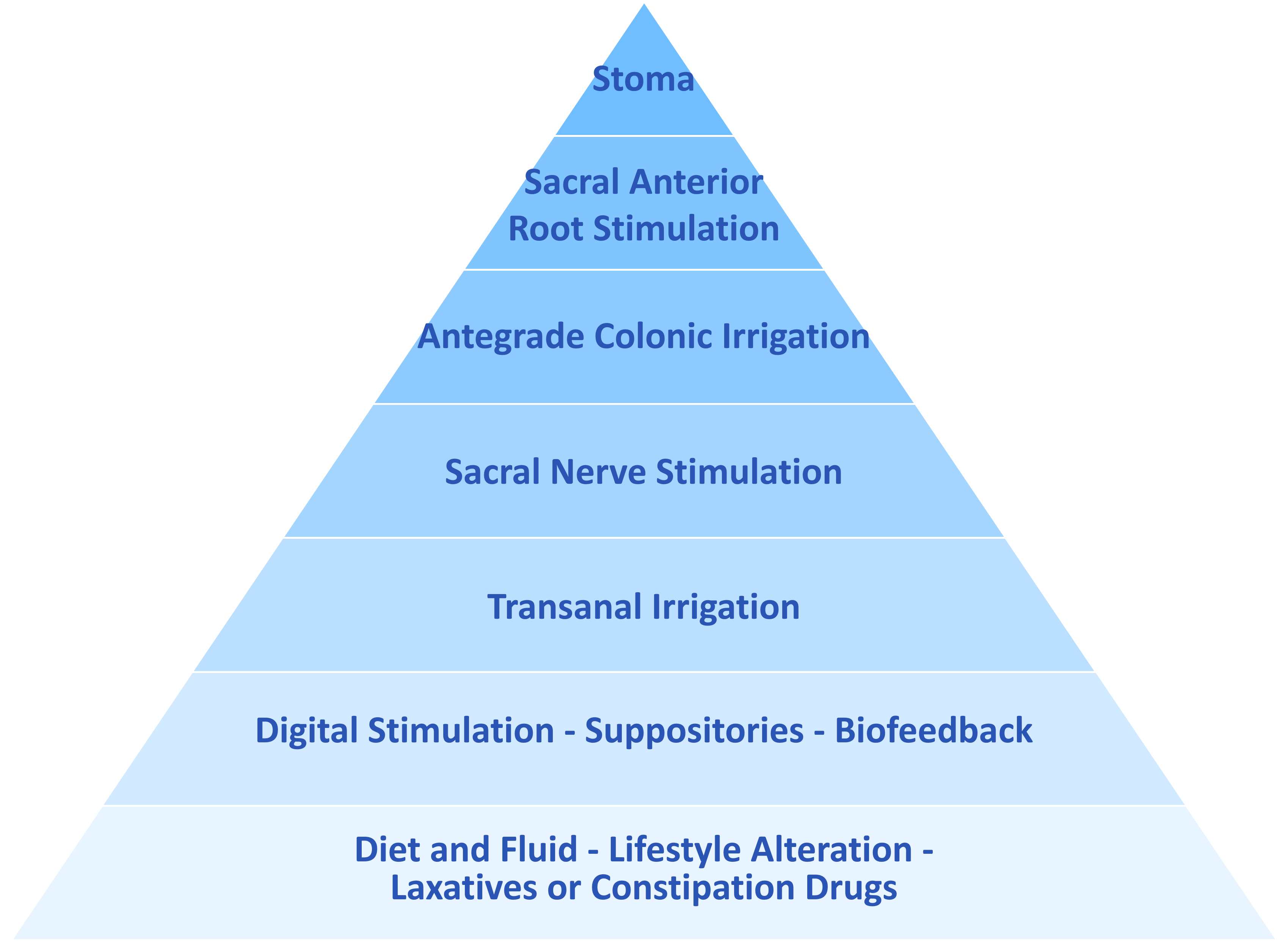
Treatments should be offered in line with the Bowel management pyramid.
Lifestyle modifications
To achieve an effect treatment, adherence not only to drugs but also diet and lifestyle changes requires understanding and acceptance to the therapy.
Pharmacological treatments
All medications, whether oral preparations or rectal suppositories should only be prescribed to treat assessment findings. It is vital to differentiate between stool softeners, stimulant laxatives, bulk forming laxatives and osmotic laxatives. Response rates with laxative treatment are estimated at around 20-40%, in randomised clinical trials, and adherence to laxatives is poor.
Biofeedback treatment has been proven to be more effective than laxatives for constipation in patients that have pelvic dyssynergia.
Treatment pathways must start with conservative treatments as described above. However, patients with STC do not respond to medical treatments. There are some small studies suggesting non-pharmacological treatments such as biofeedback, TAI, and acupuncture may be effective. The diagnosis of STC is often not established until these steps have been shown to be ineffective. For those patients not responding to conservative treatments there are a variety of surgical approaches for STC.
Transanal irrigation
Transanal irrigation is a good treatment for management of primary and secondary constipation. This treatment has been shown to provide regular and predictable bowel movements, improve quality of life and allow the individual to manage their own bowel regime.
Transanal irrigation has also been shown to be successful for some patients with STC even though there might be a risk that the large bowel wall is less prone to respond to the stimuli of irrigation in those with severe and chronic constipation.